A Look into the Brains of Babies: Functional Brain Imaging Techniques
Studying the brains of young children is not a very easy task. There are many circumstances we must consider, from applicability of a certain brain imaging technique for our young participants, to interpretability of the data we obtain. In the present article, six brain imaging techniques are introduced: fetal neurosonography, resting-state fMRI in the uterus, resting-state fMRI in babies, EEG, fNIRS and MEG. Their advantages and challenges are explained while highlighting the importance of finding balance among them. Also, a subchapter on preparation procedure for babies in fMRI (and their caregivers) is added and the safety of all the included techniques is considered. The knowledge about the infant’s brain activity can give us an insight into development of children’s behaviour, observable in the future.
Why should we study the brains of babies?
Studying various areas of child development cannot be done without considering the ways by which we can explore neural functioning in their brain. Underlying brain activity is reflected in observable behaviour of children, starting from their earliest interactions with the world around them. These behaviours can also indicate potential mental health challenges in their future, so knowing about the underlying brain divergency is key to a multidisciplinary approach. By learning about different techniques by which we can measure the brain activity of babies, we can extend our scope of methodologies that can be applied to study their behaviour more in-depth, both in research and clinical settings. In the present article, a few most common and most promising brain imagining techniques are introduced and their usefulness is explained in terms of their applicability for young children (throughout the article termed “babies”): fetuses (from 9 gestational weeks to birth), neonates (aged 0 to 2 months), infants (aged 2 to 11 months) and toddlers (aged 1 to 3 years).
Fetal brain: Ultrasound and fetal neuronosography
Our brain starts to develop in the third gestational week (Stiles & Jernigan, 2010). From the ninth gestational week on, we talk about the fetal period of human development, as the brain evolves from a smooth, “lissencephalic” structure into a mature-like gyrally and sulcally folded structure under the influence of extensive cellular changes and neuron migrations. From the fetal period on, we can attempt to study human brain functioning.
A method that allows us to observe the state of development of the fetal brain and the central nervous system as well as examine them for possible defects is fetal ultrasound which creates images of various body parts of a fetus while in womb (Johns Hopkins Medicine, 2022). Since 1996, a subtype of fetal ultrasound, fetal neurosonography, has been used. It is a technique involving multiplanar analysis of the fetal brain structures (Timor-Tritsch & Monteagudo, 1996), which means that we can look at the brain in different planes (usually in frontal, sagittal and horizontal plane). When performed by properly trained professionals using high-resolution ultrasound, fetal neurosonography gives us a detailed analysis of the cerebral anatomy, similarly accurate as the one of fetal MRI (Malinger et al., 2006). To sum up, fetal neurosonography enables us to observe the structure of the fetal brain and inspect for possible abnormalities that may reflect in the cognition of a child once born. It is used for medical diagnostics and not as much in psychological testing context, however, it gives us an insight into a basis for potential future deficits in children’s behaviour. Several mental health problems are associated with differences in size of certain brain structures. For example, the size of corpus callosum, which can be visualised on fetal neurosonography from the 18th week of gestation on, has been linked to schizophrenia, autism, and obsessive-compulsive disorder (Whittle et al., 2020). Although these mental health disorders are much more complex, these findings can help us to some extent to intervene preventively much earlier than with psychological testing later during childhood. Although fetal neurosonography gives us information on structural changes of the fetal brain, it cannot track information on its activity.
Figure 1
Fetal neurosonography scan of the brain of a fetus
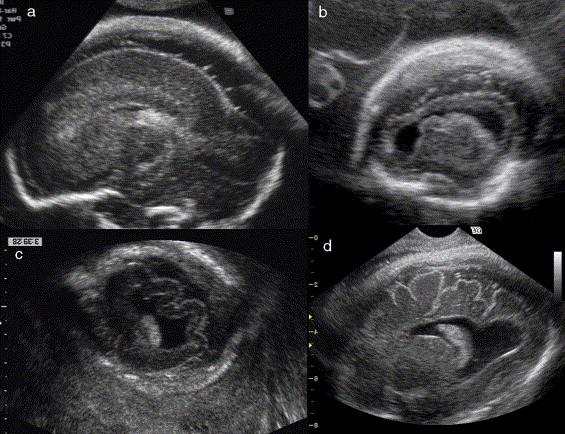
Note. From European Journal of Radiology, by G. Malinger, D. Lev and T. Lerman-Sagie, 2006, (https://ars.els-cdn.com/content/image/1-s2.0-S0720048X05003876-gr4.jpg)
Fetal brain: Resting-state fMRI in uterus
Functional magnetic resonance imaging (fMRI) is a technique based on differences in the blood flow among various brain regions. When certain brain cells are active, there is an increase of oxygenated blood which flows to that region. As oxygenated blood have different magnetic properties than deoxygenated one, a difference between this oxygenated area and other deoxygenated areas can be observed. We obtain blood-oxygenation-level-dependent (BOLD) signal, telling us which region was active (or supressed) by the flow of oxygenated blood running to it (or away from it). That way we can observe brain activity in cortical and subcortical regions of the brain. Location wise fMRI gives us excellent data, but time wise the procedure of taking images at once takes few seconds, therefore, we cannot use fMRI for rather fast processes (Ramani, 2018).
The pioneering research on fetal brain functional imaging in the uterus was done a decade and a half ago. A study by V. Schöpf and her team (2011) showed that resting-state (our brain is in a resting-state when we do nothing, and it gives us a valuable information on functional brain connectivity, so which brain areas are “wired” together and, hence, “fire” together) is present in brains of fetuses, aged 20 to 36 weeks, and that it is possible to scan it using functional magnetic resonance imaging (fMRI). Unfortunately, this study had a huge dropout due to movement of fetuses, but other later studies continued the search and found out that age-related changes in connectivity of the fetal brain in the uterus can be tracked and the pattern of activity becomes stronger with each passing week of pregnancy (Thomason et al., 2013; Turk et al., 2019). For example, the connectivity between temporal lobe on the left hemisphere and temporal lobe on the right hemisphere can be observed and it gets gradually stronger from 20th to 40th week (Thomason et al., 2013).
As we can see, it is possible to investigate some functions of fetal brain, though it is a complicated task as movement of a fetus is mostly unpredictable and can greatly blur the image we want to obtain. However, it gives us a sense of what scanning in a few weeks’ time might reveal about newborn’s brain function.
Figure 2
Fetal fMRI, coronal (left) and sagittal (right) perspectives
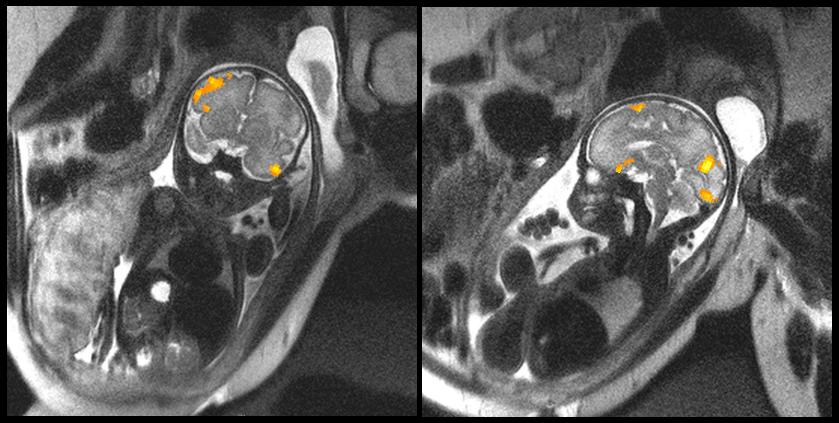
Note. From Science, by G. Miller and M. E. Thomason, 2021, https://www.science.org/do/10.1126/science.aal0587/full/ximage-1644966030463.jpg)
Baby brain: Resting-state fMRI
Once children are born, it is much more feasible to track their brain activity as they are not constantly floating in amniotic fluid in unpredictable positions. The properties of the fMRI scanner, such as its noise and narrowness, hardly make babies comfortable for participating in e.g. cognitive tasks that older children and adults can undertake, as they cannot keep still, follow instructions, give verbal responses or not get upset in such a setting (Ellis & Turk-Browne, 2018). However, we can apply resting-state functional magnetic resonance imaging (rs-fMRI) to newborns, even those aged only a few days (Kamps et al., 2020), during one of their favourite tasks: sleeping.
By studying the brains of newborns, we can answer one of the most interesting questions on human brain development: to what extent do adult brain functions emerge with development. There is a suggestion that some domain-specific networks are pre-wired and already in place even before being fully functional (Kamps et al., 2020). One study in 6- to 57-day-old newborns (mean age: 27 days) used resting-state fMRI to answer that. It was found that some cortical networks already show domain-specific patterns of functional connectivity despite the early age of babies. That was the case for the networks that later develop into strong face and scene selectivity (Kamps et al., 2020).
However, Zhang and colleagues (2019) highlight that baby resting-state might greatly differ from the resting-state of adults and that the image analysis tools for babies must consider these differences. For example, as the size of the baby brain is smaller, the voxel dimensions used for the adult brain have to be scaled down. We can also see differences in contrasts of the T1 image (one of the “black-and-white” images we obtain from fMRI scanner as a result of protons in different compounds relaxing to their original states at different speeds). T1 image of baby brain until 6 months of age appears as an inverted T1 image in adults (in newborns, grey matter looks light and white matter looks dark) and T1 image of 6- to 9-month-olds is even considered “isointense” (grey and white matter are both of a similar shade of grey colour, so the contrast is almost unnoticeable) and this must be taken into consideration. Furthermore, the artifacts that appear in the data are different (e.g., respiratory artefacts as respiratory rate in babies is faster than in adults). Despite that, the authors assume that using resting-state fMRI and developmental connectome for studying variety of early infant behaviour could be one of the shining research methodologies in the years to come (Zhang et al., 2019), as we are getting closer to know how to approach its current limitations. Therefore, it is important to consider the distinctive differences in brain functioning of babies and how they may reflect in behaviour that is psychologically observed in the first months of babies’ life after birth.
Figure 3
A baby and its fMRI scan image in the background
Note. From Emory University, by C. Inman, 2018, Earliest look at newborns’ visual cortex
reveals the minds babies are born with (https://news.emory.edu/features/2020/03/esc-newborn-visual-cortex/assets/LAK1vxSNW5/baby_fmri_images-1264×948.jpeg)
How to prepare a baby (and their caregiver) for a resting-state fMRI
It is important to know about the optimal ways of preparing babies for fMRI screening, after all, they are only a few days old little humans that have to be handled with special care. Out of all techniques mentioned in this article, fMRI has the strictest safety procedure for participants due to its magnetic and sound properties. Babies getting ready for fMRI scanning are usually swaddled and lulled to sleep, placed into a baby immobilizer for movement reduction and given earplugs and earmuffs to avoid waking up in distress while in the noisy scanner (e.g. Kamps et al., 2020). There are also some guidelines for general baby brain MRI scanning available, such as the ones by King and colleagues (2023). They suggest the following steps when in a research setting, which can be slightly modified on a case-by-case basis.
The time of scanning must be scheduled around the infant’s feeding routine, preferably with the next feeding right before the time of the scan, as parents’ arrival is suggested to be approximately an hour prior. Caregivers are offered a private quiet space where they can prepare their infant for the trial. Team members must describe the events regarding the visit and must always be available for additional questions as it is of immense importance to minimize any psychological distress of participants. (King et al., 2023)
After screening for MRI safety (such as the absence of any MR-incompatible metal implants) and before entering the scanner room, parents are encouraged to feed and hold their infants, as this increases the chances that the infant takes a full feed, falls asleep before the scan, and will remain asleep during the scan (King et al., 2023).
After the infant is fed, they are undressed to their diaper and tightly swaddled in a blanket or linen. Their arms and legs are enclosed to reduce movement. King and colleagues (2023) stated that, if preferred, the infant’s t-shirt or onesie without any metal snaps or zippers may be kept on. To protect them from MR system noise, baby-sized earmuffs are placed over the infant’s ears. They are also placed into an immobilization bag of their size. However, it still happens that babies are excluded from data analysis because of extensive motion (e.g. Kamps et al., 2020). When everything is set, the infant and caregiver are admitted to the scanner room. (King et al., 2023) The scanner in children’s laboratories is frequently plastered with fairy-tale-like motives (for example, magical trees), presumably to make it more welcoming and less intimidating for children of all ages (and their parents).
During preparation of the infant for scanning, team members can address caregivers’ concerns. Parents are typically nervous and anxious as they worry how their infant will tolerate the scan, or they want to obtain interpretable data from the MRI scan at all costs. Therefore, a careful and thorough explanation of the process is necessary. To alleviate caregiver distress, this extra time for explanations must be covered within the appointment. It is important to reassure parents that most infants sleep comfortably for the majority of the scan and in case of waking up, the caregiver can hold and soothe the infant (King et al., 2023).
Baby brain: EEG
Electroencephalography (EEG) is presumably the most common procedure for measuring brain activity. It tracks electrical activity in the cortex by electrodes placed on the scalp. This electrical activity is then tracked as an electroencephalogram and interpreted by data analysis. EEG can give us excellent information on time, but rather mediocre information on location of activity. Despite the similar way of applying EEG to adults and children, babies’ EEG recordings seem to be extremely challenging to interpret (Husain, 2005). They significantly differ from EEG recordings of older children as numerous brain features change on week-to-week basis or have different implications than in older participants (Husain, 2005). This is mostly observed in frequencies of a signal that are age specific. For example, forerunner of alpha wave (one of the waves we observe in EEG) is established at 2 months with 3- to 4-Hz frequency, at 6 months it reaches 4- to 5-Hz frequency, at 12 months it is 5- to 7-Hz and later at 3 years of age it reaches 8 Hz which falls into the typical range for alpha waves, which is 8- to 12-Hz (St Louis et al., 2016). Hence, experts must have in-depth knowledge about the brain activity of babies.
In the case of EEG studies with babies it is also important to consider the extent of motion-related artifacts in the obtained signal. Children are not used to sitting still and this is an even more significant issue in naturalistic experiments when some motion is required due to the nature of a task (Turk et al., 2022). We must also reduce duration of the session to the suggested maximum of 30 minutes for babies under 6 months (Turk et al., 2022). It is also important to consider that newborns have very thin and sensitive skin (St Louis et al., 2016), so EEG electrodes must be placed into their scalps with additional care.
Figure 4
A baby with an EEG cap

Note. From Baby & Child Research Center, 2022 (https://babyandchild.nl/wp-content/uploads/2021/09/BabyEEG3.jpg)
Baby brain: fNIRS
One of the methods that are recently gaining more attention, is functional near-infrared spectroscopy (fNIRS). It is a non-invasive technique measuring the functional activation of the human cerebral cortex as a result of oxygenation and hemodynamic changes reflecting in BOLD signal (Ferrari & Quaresima, 2012), so it measures similar changes in the brain as fMRI does. It is placed over a person’s scalp in a similar manner as EEG, but it has a better spatial resolution: while EEG can tell us where in the brain activation occurred with precision of 5–9 cm, fNIRS can give us this location information with 2–3 cm accuracy (Pinti et al., 2018). On the other hand, there seems to be a wide range of behaviours, situations, and mental processes which we cannot examine by fMRI due to its weaker temporal resolution: fMRI can only give us information on time of occurrence of an activity in precision of seconds, fNIRS in hundredths of a second (Pinti et al., 2018). fNIRS therefore enables better spatial resolution than EEG and better temporal resolution than fMRI while also having a very good robustness to motion (Pinti et al., 2018). The positioning of a cap with optodes in fNIRS is relatively easy and fibber optic cables, connecting optodes with the rest of the system, can be placed so that they do not intervene with the child’s movement (and the movement of these cables does not induce artefacts which happens with EEG) (Nishiyori, 2016).
As fNIRS is portable, easy to apply and has a relatively good tolerance to movement, it is a very relevant method for younger children (Gallagher et al., 2023). fNIRS can also be used repeatedly and for long periods of time while its setup allows for larger body movement compared to traditional techniques (Nishiyori, 2016), such as fMRI and EEG.
Despite that, fNIRS is not that commonly used and there is a lack of standardization in data analysis (Pinti et al., 2018). Additionally, near-infrared lights can only reach the surface of the cortex, not the deeper brain structures (Kao & Zhang, 2019) which also applies to EEG. Nevertheless, it has potential to become even more used than EEG. As it can be applied to wide range of populations in their everyday environments and can be interfaced with other methodologies, e.g. eye-tracking or breathing rate, it can pave the new ways of cognitive and developmental research in the following decades (Pinti et al., 2018), especially in the population of children. By using it, we can study the neural basis of behaviours that we cannot study that well by using other techniques, such as the emergence of goal-directed actions in infants (Nishiyori, 2016). Hence, Nishiyori (2016) also speculates that fNIRS has a lot of possible implications in developmental research of movement in children.
Figure 5
A baby with fNIRS cap

Note. From Artinis Medical Systems, 2024 (https://static1.squarespace.com/static/64e314a8c69b933a41187ec2/64e35516dd49cb34bbf316e6/64e3560b76da863ebb524121/1715959402298/BabyBrite%2Btwins-92.jpg?format=1500w)
Baby brain: MEG
Another technique used is magnetoencephalography (MEG). MEG on its own measures changes in magnetic field on smaller areas scattered around the whole brain. If certain brain cells are active, there will be an increase in the magnetic field around them and magnetic sensors, that are cooled down to very low temperatures inside the machine, detect this increase. When we combine it with a three-dimensional head model from a participant’s magnetic resonance imaging (MRI) scan, MEG becomes functional magnetic source imaging (MSI) (Kao & Zhang, 2019). That way MEG can give us excellent information on the time and location of activity. As MEG is less sensitive to conductivity differences between the brain, cerebral spinal fluid, skull, and scalp, it gives us more precise information about the source localization of activity in comparison to EEG (Chen et al., 2019).
Infant whole-head MEG systems have only recently been developed (Chen et al., 2019), but there seems to be a broad spectre of possible research questions for which MEG in combination with an MRI scan of an infant’s brain can give us answers to, for example how bilingualism shapes baby brain (Ferjan Ramírez et al., 2016). Mostly it could be used for cognitive tasks, as MEG setup is not moveable, but there are also attempts to design wearable systems (Chen et al., 2019). One of them, optically pumped magnetometer MEG (OPM-MEG), seems to be a more practical and enhanced alternative to MEG, far more accessible to children in the form of a wearable helmet (UCL, 2021).
However, MEG is expensive and not many research centres can afford it for now. Those that do, see its benefits in its temporal precision that can be applied to a three-dimensional MRI model of the brain with great spatial precision.
Figure 6
A baby during MEG scan

Note. From Institute for Learning & Brain Sciences, 2024, (https://ilabs.uw.edu/wp-content/uploads/2021/10/BabyInMEG_400.png).
Figure 7
A child wearing an OPM-MEG helmet

Note. From UCL, 2021 (https://www.ucl.ac.uk/news/sites/news/files/styles/large_image/public/opm_meg_helmet_8x5.jpg?itok=mK9bHDFa).
Safety of these techniques for children
These brain imaging techniques, such as fetal neurosonography (Whittle et al., 2020), EEG (Husain, 2005), fNIRS (Pinti et al., 2018) and MEG (Chen et al., 2019) are mostly seen as safe for use in children. A safety concern that had be raised is one regarding fMRI use because the machine itself is quite loud, even if you are in a womb, therefore, it is reasonable to speculate it could potentially be hazardous for fetal hearing. However, studies did not find an increase in the rate of hearing abnormalities or fetal growth in general in healthy babies when exposed to in uterus MRI at any gestational age (Jaimes et al., 2018; Chartier et al., 2019). Still, earmuffs are essential in baby MRI and fMRI scanning (King et al., 2023), so it can be assumed that they do not only keep an infant asleep but also provide additional hearing damage prevention. Nevertheless, from what we know so far, it seems safe to use all the above-mentioned brain scanning techniques.
Comparison of techniques in terms of suitability for children research
Most of the characteristics that serve as advantages and challenges of brain imaging research in adults are also present in baby research. We usually focus on two criteria: spatial resolution (i.e., how precisely we can determine where locationally some activity in the brain occurred) and temporal resolution (i.e., how precisely we can determine when in time it happened). By the latter criterion, fNIRS, EEG and MEG all give us excellently precise information in time, even not so optimal temporal resolution of fMRI, which is around few seconds, can be suitable for some types of research, such as sleep research using rs-fMRI. From the perspective of spatial resolution, fMRI or MSI (MEG combined with MRI brain model) would be the best fit as other techniques mostly rely on approximations calculated by the position of electrodes.
On the other hand, probably the most significant criterion for baby brain research and suitability of brain imaging techniques in children is mobility of the setup and the participant within it. Regarding mobility, MEG and fMRI are stable machines we cannot use outside a laboratory. In both scanners, children cannot move freely, for example, crawl around, but MEG is only in contact with the participant’s head, so an infant can potentially move their arms which they cannot do in an MR machine. Fetal neurosonography could also fall into the less-mobile group of techniques because the movement of a fetus can result in blurred pictures that cannot be used for analysis (same applies to fetal fMRI). On the other hand, EEG and fNIRS are the most mobile and infant-friendly systems (Turk et al., 2022). They both allow participants to move around, yet fNIRS has a better motion tolerance than EEG and better spatial resolution. Therefore, fNIRS seems like a promising technique for measuring the brain activity of babies in movement.
In addition to all, it is usually the nature of our research topic and availability of techniques that determine which technique we use. Not all techniques are financially available for all research, for example, the MEG machine is very expensive, and its installation is quite complicated because of its weight. Meanwhile, EEG setup costs only a few (ten) thousands of euros and can be much easily stored. Money and place concerns aside, we first must consider the age group of our participants and apply techniques suitable for them. For example, if we want to observe fetal brain activity, we have to rely on fetal fMRI, but if we are only interested in fetal brain structure, we may use fetal neurosonography. After that we must consider what kind of behaviour we can expect infants to be able to carry out during scanning, mostly meaning, if it is enough for them to only sleep or if we would like to access their brain activity during some other tasks. For example, if we want to observe an infant taking their first steps by walking, we will probably use fNIRS for its mobility and motion tolerance. If we want to observe an infant in their interaction with a parent during reading a story, we could use MEG to track activity and combine it with MRI scan for MSI. Then, we must ask ourselves which technique will enable us to track the phenomenon as it occurs best. For example, if we want a precise information on location of some rapid occurring activity in the brain, we will not use fMRI (because of its lower temporal resolution), nor EEG (because of its lower spatial resolution) but we might use other techniques that ticked the boxes of previously stated criteria. Finally, it is important to take into consideration the fact that triangulation of methods (i.e., using more than just one method) gives us the most informative conclusions if we combine them purposefully.
Conclusion
As we can see, studying the brains of young children has recently become a much more interesting area of research due to technological advancements in brain imaging techniques and their suitability for use in infant population. Nevertheless, not many studies are done using these techniques, although they could give a profound knowledge on baby brain development that later reflects in behaviour, cognition and mental health of older children and adults. By expanding our horizons about methodologies, we can contribute to more informative and quality research on the brains of infants. This can then translate into clinical settings and enable better preventive and curative interventions for psychological well-being of children.
Literature
Artinis Medical Systems. (2024, May 17). Exploring the infant brain with fNIRS — Artinis Medical Systems | (f)NIRS devices. [Photograph] Artinis Medical Systems | (F)NIRS Devices. https://www.artinis.com/blogpost-all/2021/exploring-the-infant-brain-with-fnirs
Baby & Child Research Center. (2022, January 5). Hersenactiviteit meten – Baby & Child Research Center. [Photograph] Baby & Child Research Center. https://babyandchild.nl/wp-content/uploads/2021/09/BabyEEG3.jpg
{kind=link}
Chartier, A. L., Bouvier, M. J., McPherson, D. R., Stepenosky, J. E., Taysom, D. A., & Marks, R. M. (2019). The safety of maternal and fetal MRI at 3 T. American Journal of Roentgenology, 213(5), 1170–1173. https://doi.org/10.2214/ajr.19.21400
Chen, Y.-H., Saby, J., Kuschner, E., Gaetz, W., Edgar, J. C., & Roberts, T. P. L. (2019). Magnetoencephalography and the infant brain. NeuroImage, 189, 445–458. https://doi.org/10.1016/j.neuroimage.2019.01.059
Clark, C., & Inman, C. [Photographer]. (2018). Earliest look at newborns’ visual cortex reveals the minds babies are born with. Emory University. https://news.emory.edu/features/2020/03/esc-newborn-visual-cortex/index.html
Ellis, C. T., & Turk-Browne, N. B. (2018). Infant fMRI: A model system for cognitive neuroscience. Trends in Cognitive Sciences, 22(5), 375–387. https://doi.org/10.1016/j.tics.2018.01.005
Ferjan Ramírez, N., Ramírez, R. R., Clarke, M., Taulu, S., & Kuhl, P. K. (2016). Speech discrimination in 11‐month‐old bilingual and monolingual infants: A magnetoencephalography study. Developmental Science, 20(1). https://doi.org/10.1111/desc.12427
Ferrari, M., & Quaresima, V. (2012). A brief review on the history of human functional near-infrared spectroscopy (FNIRS) development and fields of application. NeuroImage, 63(2), 921–935. https://doi.org/10.1016/j.neuroimage.2012.03.049
Gallagher, A., Wallois, F., & Obrig, H. (2023). Functional near-infrared spectroscopy in pediatric clinical research: Different pathophysiologies and promising clinical applications. Neurophotonics, 10(02). https://doi.org/10.1117/1.nph.10.2.023517
Husain, A. M. (2005). Review of neonatal EEG. American Journal of Electroneurodiagnostic Technology, 45(1), 12–35. https://doi.org/10.1080/1086508x.2005.11079505
Institute for Learning & Brain Sciences (2024). Future use of MEG. [Photograph] University of Washington. https://ilabs.uw.edu/wp-content/uploads/2021/10/BabyInMEG_400.png
{kind=link}
Jaimes, C., Delgado, J., Cunnane, M. B., Hedrick, H. L., Adzick, N. S., Gee, M. S., & Victoria, T. (2018). Does 3-T fetal MRI induce adverse acoustic effects in the neonate? A preliminary study comparing postnatal auditory test performance of fetuses scanned at 1.5 and 3 T. Pediatric Radiology, 49(1), 37–45. https://doi.org/10.1007/s00247-018-4261-2
Johns Hopkins Medicine. (2022, January 26). Fetal ultrasound. https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/fetal-ultrasound
Kamps, F. S., Hendrix, C. L., Brennan, P. A., & Dilks, D. D. (2020). Connectivity at the origins of domain specificity in the cortical face and place networks. Proceedings of the National Academy of Sciences, 117(11), 6163–6169. https://doi.org/10.1073/pnas.1911359117
Kao, C., & Zhang, Y. (2019). Magnetic source imaging and infant meg: Current trends and technical advances. Brain Sciences, 9(8), 181. https://doi.org/10.3390/brainsci9080181
King, R., Low, S., Gee, N., Wood, R., Hadweh, B., Houghton, J., & Leijser, L. M. (2023). Practical stepwise approach to performing neonatal brain MR imaging in the research setting. Children, 10(11), 1759. https://doi.org/10.3390/children10111759
Malinger, G., Lev, D., & Lerman-Sagie, T. (2006). Normal and abnormal fetal brain development during the third trimester as demonstrated by neurosonography. European Journal of Radiology, 57(2), 226–232. https://doi.org/10.1016/j.ejrad.2005.11.022
Miller, G., & Thomason, M. E. [Photo owner]. (2021, October 18). Pioneering study images activity in fetal brains. AAAS Articles DO Group. https://doi.org/10.1126/science.aal0587
Nishiyori, R. (2016). FNIRS: An emergent method to document functional cortical activity during infant movements. Frontiers in Psychology, 7. https://doi.org/10.3389/fpsyg.2016.00533
Pinti, P., Tachtsidis, I., Hamilton, A., Hirsch, J., Aichelburg, C., Gilbert, S., & Burgess, P. W. (2018). The present and future use of functional near‐infrared spectroscopy (FNIRS) for Cognitive Neuroscience. Annals of the New York Academy of Sciences, 1464(1), 5–29. https://doi.org/10.1111/nyas.13948
Ramani, R. (2018). Functional MR Imaging. In Elsevier eBooks (pp. 299–326). https://doi.org/10.1016/b978-0-12-809915-5.00011-5
Schöpf, V., Kasprian, G., Brugger, P. C., & Prayer, D. (2011). Watching the fetal brain at ‘rest.’ International Journal of Developmental Neuroscience, 30(1), 11–17. https://doi.org/10.1016/j.ijdevneu.2011.10.006
St Louis, E. K., Frey, L. C., Britton, J. W., Frey, L. C., Hopp, J. L., Korb, P., Koubeissi, M. Z., Lievens, W. E., Pestana-Knight, E. M., & St Louis, E. K. (2016). The developmental EEG: premature, neonatal, infant, and children. Electroencephalography (EEG): An Introductory Text and Atlas of Normal and Abnormal Findings in Adults, Children, and Infants – NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK390356/
Stiles, J., & Jernigan, T. L. (2010). The basics of Brain Development. Neuropsychology Review, 20(4), 327–348. https://doi.org/10.1007/s11065-010-9148-4
Thomason, M. E., Dassanayake, M. T., Shen, S., Katkuri, Y., Alexis, M., Anderson, A. L., Yeo, L., Mody, S., Hernandez-Andrade, E., Hassan, S. S., Studholme, C., Jeong, J.-W., & Romero, R. (2013). Cross-hemispheric functional connectivity in the human fetal brain. Science Translational Medicine, 5(173). https://doi.org/10.1126/scitranslmed.3004978
Timor-Tritsch, I. E., & Monteagudo, A. (1996). Transvaginal fetal neurosonography: Standardization of the planes and sections by anatomic landmarks. Ultrasound in Obstetrics and Gynecology, 8(1), 42–47. https://doi.org/10.1046/j.1469-0705.1996.08010042.x
Turk, E., Endevelt-Shapira, Y., Feldman, R., van den Heuvel, M. I., & Levy, J. (2022). BRAINS IN SYNC: Practical guideline for parent–infant EEG during natural interaction. Frontiers in Psychology, 13. https://doi.org/10.3389/fpsyg.2022.833112
Turk, E., Van Den Heuvel, M. I., Benders, M. J., De Heus, R., Franx, A., Manning, J. H., Hect, J. L., Hernandez-Andrade, E., Hassan, S. S., Romero, R., Kahn, R. S., Thomason, M. E., & Van Den Heuvel, M. P. (2019). Functional connectome of the fetal brain. the Journal of Neuroscience/the Journal of Neuroscience, 39(49), 9716–9724. https://doi.org/10.1523/jneurosci.2891-18.2019
UCL. (2021, October 4). Wearable brain scanner to facilitate testing for children with. UCL News. https://www.ucl.ac.uk/news/2021/oct/wearable-brain-scanner-facilitate-testing-children-epilepsy ; [Photograph] https://www.ucl.ac.uk/news/sites/news/files/styles/large_image/public/opm_meg_helmet_8x5.jpg?itok=mK9bHDFa
{kind=link}
Whittle, S., Finn, M., Little, K., & Olsson, C. A. (2020). A methodological review of Fetal neurosonographic studies: New Directions in assessment of neurodevelopmental risk for mental health problems. Neuroscience & Biobehavioral Reviews, 114, 172–193. https://doi.org/10.1016/j.neubiorev.2020.03.031 Zhang, H., Shen, D., & Lin, W. (2019). Resting-state functional MRI studies on infant brains: A decade of gap-filling efforts. NeuroImage, 185, 664–684. https://doi.org/10.1016/j.neuroimage.2018.07.004


You May Also Like

Razumevanje depresije v športu

Umetnost – umirjenost in užitek: potencial estetskega doživetja za spodbujanje pozitivnega čustvovanja
